Preventing diabetic foot ulcers and amputations
June 27, 2026

Diabetic foot ulcers are a common and serious complication of diabetes. In Malaysia, the local prevalence of diabetic foot infections increased from 11.6% in 2006 to 17.5% in 2015. Globally, an estimated 589 million adults were living with diabetes in 2024, according to the International Diabetes Federation.
The consequences of diabetic foot ulcers are severe. Approximately 50% of patients die within five years of developing a diabetic foot ulcer, while the mortality rate rises to 70% within five years following a major lower-limb amputation. In Malaysia, the cost of managing Type 2 diabetes was estimated at RM1.40 billion in 2011, accounting for more than 9% of the Ministry of Health's total budget. Furthermore, 80% of non-traumatic lower-limb amputations in people with diabetes are preceded by a foot ulcer. Pathophysiology of diabetic foot infections Diabetic neuropathy is one of the main contributors to diabetic foot ulcer development.
Metabolic dysfunction Persistent hyperglycemia reduces blood supply to peripheral nerves and promotes inflammation through activation of the polyol pathway, oxidative stress and protein kinase C (PKC). These processes contribute to peripheral nerve damage and vascular injury. "Manage hyperglycemia. Somehow or other, you have to try and reduce the glucose that gets into the system. After that you can talk about whether the blood vessels are affected or whether the nerves are affected. "The reason why even a simple ulcer develops is mainly because sensation is lost. Somehow or other, the sensation in the foot is affected first. "Our hands have far greater sensory discrimination than our feet. If you are given an apple and an orange, your hands can easily distinguish between them simply by touch. Your feet cannot do that because sensation is naturally less refined. When diabetes further reduces sensation in the feet, the risk of unnoticed injuries increases significantly," explains Dr Thaveethu Moses (pixture below), Consultant Orthopedic Surgeon, during Assunta Hospital's GP Symposium: Diabetes 360 – A Multidisciplinary Approach for GPs. 
Diabetic angiopathy
Hyperglycemia causes endothelial damage, dyslipidemia and chronic inflammation, accelerating atherosclerosis. Peripheral vascular constriction and hypercoagulation reduce blood flow, resulting in ischemia and delayed wound healing. "The loss of sensation means patients cannot accurately judge how much damage they are causing to their feet. At the same time, elevated blood sugar weakens the immune system. When poor sensation, reduced blood flow and impaired immunity occur together, the foot becomes highly susceptible to infection," he says. Immune dysfunction Diabetes also impairs the body's ability to fight infection by causing:
"You manage the hyperglycemia and you manage the blood flow. One of the simplest ways to improve blood flow is by walking. Regular walking creates a demand for new blood vessels to develop. "Given enough time and consistent exercise, blood supply can improve remarkably. By improving blood flow alongside glucose control, patients can also improve their symptoms," adds Dr Moses. IDSA/IWGDF classification of diabetic foot infection The Infectious Diseases Society of America (IDSA) and the International Working Group on the Diabetic Foot (IWGDF) classify diabetic foot infections into four grades:
Recognizing local infection Clinical signs include:
Recognizing systemic inflammatory response syndrome (SIRS) Patients should be assessed for:
Early-stage management According to Dr Moses, early-stage disease can often be managed conservatively. "Stage 1 and Stage 2 patients usually do not require hospital treatment. They may simply need nail trimming, callus care and, in selected cases, antibiotics." In Stage 1 disease, patients typically have only a callus or pressure-related hardened skin. Antibiotics are generally unnecessary unless infection is present. Proper callus removal is essential because untreated calluses eventually crack, exposing the underlying skin and creating an entry point for bacteria. Dressing the wound Dr Moses emphasizes that wound dressing has become much simpler than in the past. Modern wound care options include honey dressings, negative-pressure wound therapy (vacuum dressings), hyperbaric oxygen therapy and maggot therapy. However, effective wound care does not necessarily require expensive products. The priority is maintaining strict aseptic technique. Key principles include:
Preventing pressure-related ulcers Dr Moses stresses that pressure is the primary mechanical factor leading to ulcer formation. If one fourth toe develops an ulcer due to shoe pressure, the corresponding toe on the opposite foot may also be at risk because of similar foot anatomy and footwear habits. "This is usually caused by wearing closed shoes that place pressure on the toe. Patients do not necessarily need expensive diabetic footwear or custom orthotics. Often, a simple pair of well-fitting strap sandals that avoids pressure over the affected toe is sufficient." He adds that ingrown toenails can also create pressure, leading to ulcers and infection. Early toenail management, including nail removal when necessary, can often be performed safely in the clinic. Antibiotic therapy Dr Moses notes that ampicillin/sulbactam (Unasyn) is commonly used as an empirical antibiotic for diabetic foot infections because of its broad-spectrum antimicrobial coverage. He explains that it provides good bioavailability, is effective against many common pathogens responsible for diabetic foot infections and is available in oral formulations, making it a practical treatment option in appropriate patients. |
EXPLORE FURTHER
|
Diabetes linked to higher gallbladder disease riskRecognizing hidden warning signs before serious pancreatic and biliary complications
|

|
Infants of diabetic mothers: Causes and complicationsPoor maternal glucose control during pregnancy heightens lifelong neonatal metabolic complications
|

|
Interpreting skin signs in diabetesEarly skin changes may signal hidden complications and poor glycemic control
|
|
Ethnic variations in glycaemic response to simple sugars and carbohydratesImpact on blood glucose levels in Caucasians versus Asians
|
|
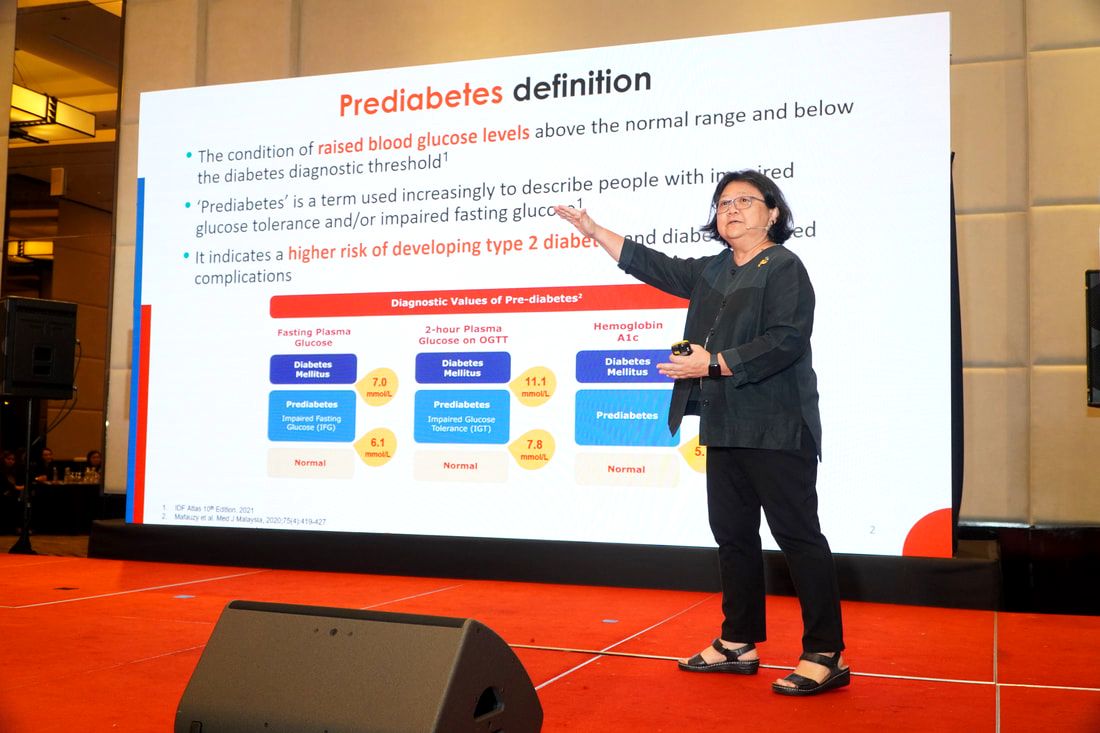
One in 10 prediabetic individuals progress to diabetes within a yearLimitations of finger prick testing for prediabetes diagnosis
|

|
Teh tarik vs. teh O: The struggle every diabetes patient face!Managing carbohydrates to prevent hypoglycemia
|
|
Not so sweet: The connection between erectile health and diabetesDiabetes increases the risk of developing ED 3.5 times
|

|
Women with pre-term delivery, gestational diabetes and rheumatoid arthritis at higher risk of heart diseaseThree times at higher risk of cardiovascular deaths
|

|
Diabetes: Subtle signs you should not ignoreSubtle signs include urinating often, thirsty, urinary tract infection, weight...
|

|
Diabetic retinopathy: A common cause for blindness in adultsThe most common eye disease
|

|
Empowering children with type 1 diabetes mellitusIs complete avoidance of sweets and sugar the solution?
|

|
Can diabetes be reversed?Discover the power to reverse diabetes through nutrition and lifestyle
|

|
Maggot debridement therapy: Rescuing limbs from amputationAn innovative modality for the treatment of chronic wounds
|

|
Diabetes treatments continue to evolveGlucagon-like-peptide-1 receptor agonists increases the secretion of insulin
|